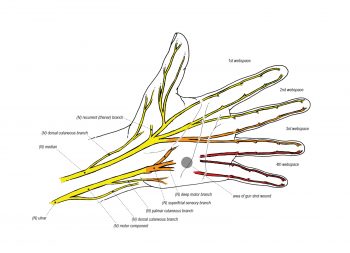
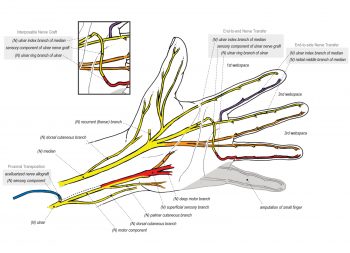
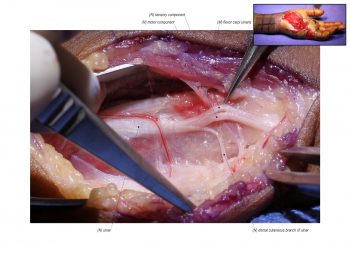
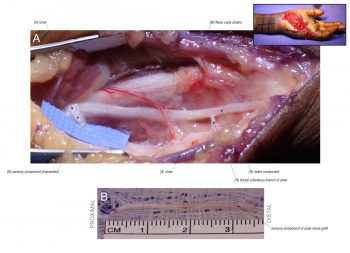
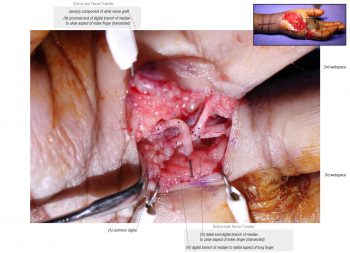
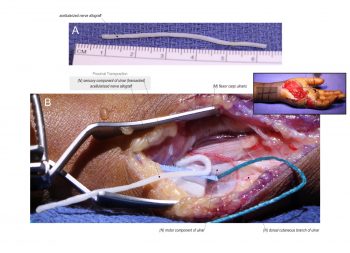
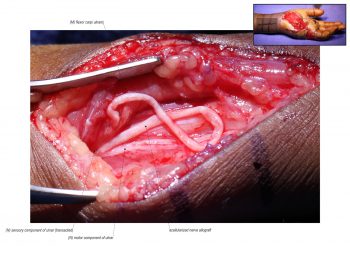
For distal sensory ulnar nerve injuries in the hand, there is an alternative approach in restoration of critical ulnar nerve sensation. In this case, the patient had a gunshot wound and required amputation of the small finger. As result, the ulnar aspect of the ring finger became the critical target for sensory reinnervation. In addition, soft tissue coverage of the palm was an obstacle for long nerve grafts. Goals were to restore critical sensation and prevent painful neuroma formation. The median nerve branch to the ulnar aspect of the index finger was used as the donor nerve to reinnervate the recipient ulnar nerve branch to the ulnar aspect of the ring finger. A nerve graft was required to bridge the distance and the ulnar sensory fascicle proximal to the injury was harvested as expendable graft material. An acellularized nerve allograft is used to extend the proximal end of the ulnar sensory fascicle for proximal transposition. To preserve rudimentary sensation to the donor nerve, an end-to-side nerve transfer to the lateral aspect of the long finger is completed.
Standard 110817
Extended 110817
POSITION
Supine.
INCISION
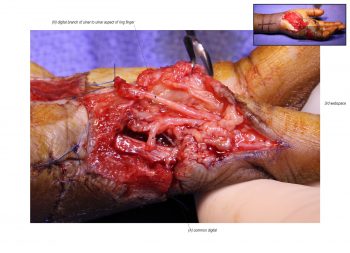
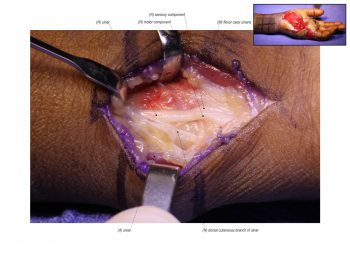
The reconstruction of critical ulnar ring finger sensation involves multiple incisions. The first incision is made on the ulnar aspect of the distal forearm to expose the ulnar nerve proximal to the area of injury. The second incision is made on the ulnar aspect of the ring finger to expose the recipient ulnar nerve. The third incision is made on the 2nd web space to the ulnar aspect of the index finger to expose the donor median nerve.
REFERENCES
- Watson CP, Mackinnon SE, Dostrovsky JO, Bennett GJ, Farran RP, Carlson T. Nerve resection, crush and re-location relieve complex regional pain syndrome type II: a case report. Pain. 2014 Jun;155(6):1168-73. PMID: 24502845.
- Boyd KU, Nimigan AS, Mackinnon SE. Nerve reconstruction in the hand and upper extremity. Clin Plast Surg. 2011 Oct;38(4):643-60. Review. PMID: 22032591.
- Fox IK, Mackinnon SE. Adult peripheral nerve disorders: nerve entrapment, repair, transfer, and brachial plexus disorders. Plast Reconstr Surg. 2011 May;127(5):105e-118e. Review. PMID: 21532404.
- Tung TH, Mackinnon SE. Nerve transfers: indications, techniques, and outcomes. J Hand Surg Am. 2010 Feb;35(2):332-41. Review. PMID: 20141906.
- Brown JM, Yee A, Mackinnon SE. Distal median to ulnar nerve transfers to restore ulnar motor and sensory function within the hand: technical nuances. Neurosurgery. 2009 Nov;65(5):966-77; discussion 977-8. PMID: 19834412.
- Brown JM, Mackinnon SE. Nerve transfers in the forearm and hand. Hand Clin. 2008 Nov;24(4):319-40, v. Review. PMID: 18928884.
- Pannucci C, Myckatyn TM, Mackinnon SE, Hayashi A. End-to-side nerve repair: review of the literature. Restor Neurol Neurosci. 2007;25(1):45-63. Review. PMID: 17473395.
- Vernadakis AJ, Koch H, Mackinnon SE. Management of neuromas. Clin Plast Surg. 2003 Apr;30(2):247-68, vii. Review. PMID: 12737355.
- Tarasidis G, Watanabe O, Mackinnon SE, Strasberg SR, Haughey BH, Hunter DA. End-to-side neurorrhaphy resulting in limited sensory axonal regeneration in a rat model. Ann Otol Rhinol Laryngol. 1997 Jun;106(6):506-12. PMID: 9199612.
- Novak CB, van Vliet D, Mackinnon SE. Subjective outcome following surgical management of lower-extremity neuromas. J Reconstr Microsurg. 1995 May;11(3):175-7. PMID: 7650641.
- Dellon AL, Mackinnon SE. Treatment of the painful neuroma by neuroma resection and muscle implantation. Plast Reconstr Surg. 1986 Mar;77(3):427-38. PMID: 2937074.



Disclosure: No authors have a financial interest in any of the products, devices, or drugs mentioned in this production or publication.