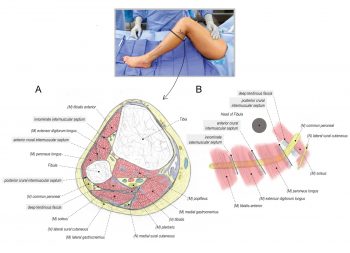
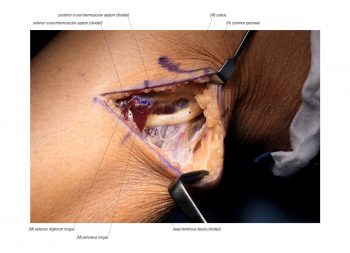
Entrapment of the common peroneal nerve (CPN) at the fibular head is an under-recognized lower extremity neuropathy that contributes to weakness of the musculature within the anterior and lateral compartments of the leg and progress to foot drop. As well, there can be numbness/pain within the territory of the superficial and deep peroneal nerve. Compression of the CPN can be attributed primarily to the posterior crural intermuscular septum found deep to the leading-edge of the peroneus longus. The anterior crural intermuscular septum and a third intermuscular septum are also associated with this compression neuropathy, as well as the surrounding fascia layer that entraps the CPN on top of the deep tendinous fascia. These structures are released to decompress the CPN at the fibular head. Motor branches from the CPN have been seen to pierce these intermuscular septums. In this case, the patient presented with a complex history of neuropathic pain in the lower left leg following multiple knee surgeries over a span of many years. During examination, the patient was able to tolerate light touch related to compression-type injury rather than withdrawing from severe pain in keeping with a neurectomy-type injury; thus compression neuropathy and not neuroma injury was suspected. The scratch collapse test with ethyl chloride revealed provocation, first at the CPN at the fibular head, then second at the saphenous nerve in the thigh, and then third at the superficial peroneal nerve. Her surgical management included the release of these three nerves. This video outlines the surgical technique for releasing the CPN at the fibular head. The lateral sural cutaneous nerve was not evident in this case.
Standard 161012
Extended 161012
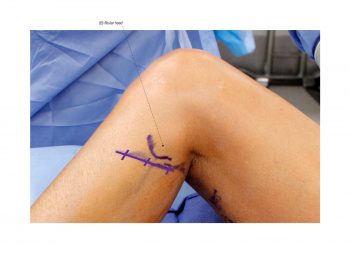
INCISION
An oblique incision is made just inferior to the fibular head and oriented from posterior-proximal to anterior-distal along the course of the common peroneal nerve.
POST-OPERATIVE MANAGEMENT
The incision is closed with absorbable suture and glue. A soft compression dressing is applied. Patients are allowed to weight-bear as tolerated. Assistive devices are offered to patients post-operatively but typically are not needed. Patients are instructed to avoid unnecessary ambulation and elevate the leg as much as possible during the first three weeks post-operatively. This will help limit swelling of the lower extremity and any issues with wound healing. Diabetic and obese patients may require additional interrupted nylon sutures to support their incision. These are removed at two weeks post-operatively. At three weeks post-operatively, patients may be referred to physical therapy to address any issues with edema, scar, ankle ROM, strength and ambulation. At two months post-operatively, they are typically released to all activities.
REFERENCES
- Gillenwater J, Cheng J, Mackinnon SE. Evaluation of the scratch collapse test in peroneal nerve compression. Hand (NY). 2015 Jun;10(2):161-7. PMID: 21681130.
- Humphreys DB, Novak CB, Mackinnon SE. Patient outcome after common peroneal nerve decompression. J Neurosurg. 2007 Aug;107(2):314-8. PMID: 17695385.

Disclosure: No authors have a financial interest in any of the products, devices, or drugs mentioned in this production or publication.